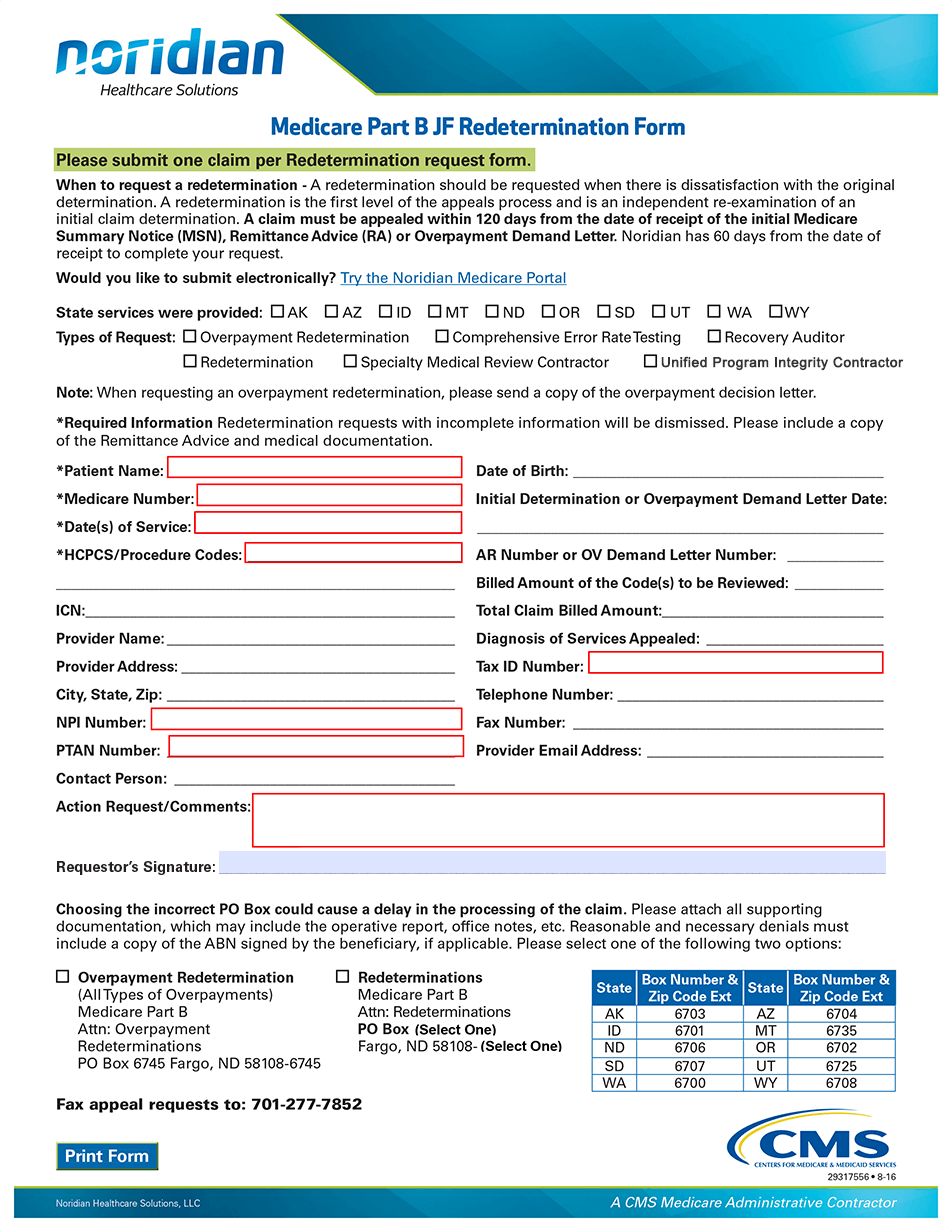
Medicare Part B Redetermination Form
Medicare Part B Redetermination Form - Use this form to appeal a medicare claim decision at the first level of appeal. Please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Download and submit this form to request a redetermination of a medicare claim within 120 days from the date of receipt of the initial determination. Cms will then provide the drug company with the. Palmetto gba is responsible for completing first. The form requires patient and provider. Select your jurisdiction, provide your provider and beneficiary information, and explain your reason for. Please submit one claim per redetermination request form. If you are unable to submit your. The penalty is 10% of $185, which is $18.50. Learn how to request an appeal (redetermination) if you disagree with medicare's coverage or payment decision. Original medicare (part a and b) eligibility and enrollment; If you wish to appeal this decision, please fill out the required information below and mail this form to the address shown below. Palmetto gba is responsible for completing. Please do not use staples for any documentation fields with a red asterisk (*) are required. The penalty is 10% of $185, which is $18.50. Download and submit this form to request a redetermination of a medicare claim within 120 days from the date of receipt of the initial determination. Download and complete this form to appeal a medicare part b claim denial. Download and complete this form to request a redetermination or clerical error reopening for medicare part b claims. Personalized choicesexpert guidancecompare medicare optionsshop plans online Use this form to appeal a medicare claim decision at the first level of appeal. For your convenience this form can. This tutorial has been created to assist you in completing the medicare part b redetermination and clerical error reopening request form (form 152). Medicare part b inflation rebate program revised guidance (pdf) (december 14, 2023). Download and submit this. You choose to reenroll in part b in 2025. Medicare redetermination request form department of health and human services centers for medicare & medicaid services 1. Trusted companiesenrollment optionsget personalized quotesfind medicare plans A redetermination is the first level of the medicare appeals process. Download and complete this form to appeal a medicare part b claim denial. Trusted companiesenrollment optionsget personalized quotesfind medicare plans Find out the timeliness, filing options, form. Trusted companiesenrollment optionsget personalized quotesfind medicare plans Download and complete this form to request a redetermination of a denied claim for medicare part b services. Download and submit this form to request a redetermination of a medicare claim within 120 days from the date of receipt. Find out the timeliness, filing options, form. The form includes provider and beneficiary information, overpayment appeal, and. Download and complete this form to request a redetermination of a denied claim for medicare part b services. This form may be used to request a redetermination for medicare part b services. Download and complete this form to appeal a medicare part b. You need to provide your name, medicare number, date of service, date of notice, and reason for. You may also submit additional evidence at a later time, but. Download and complete this form to request a redetermination of a denied claim for medicare part b services. Learn how to request a redetermination for medicare part b claims when you disagree. Download and complete this form to appeal a medicare part b claim denial. At a minimum, you must complete/ include. The penalty is 10% of $185, which is $18.50. Use this form to appeal a medicare claim decision at the first level of appeal. Cms will then provide the drug company with the. Medicare redetermination request form department of health and human services centers for medicare & medicaid services 1. Please do not use staples for any documentation fields with a red asterisk (*) are required. Download and complete this form to appeal a medicare part b claim denial. Medicare part b redetermination and clerical error reopening request form. Please complete each field. Please submit one claim per redetermination request form. Learn how to request a redetermination for medicare part b claims when you disagree with the initial determination. Medicare part b jf redetermination form. Original medicare (part a and b) eligibility and enrollment; Select your jurisdiction, provide your provider and beneficiary information, and explain your reason for. Cms will then provide the drug company with the. The form requires patient and provider. If you wish to appeal this decision, please fill out the required information below and mail this form to the address shown below. You choose to reenroll in part b in 2025. Medicare part b inflation rebate program revised guidance (pdf) (december 14, 2023). The form includes provider and beneficiary information, overpayment appeal, and. If you wish to appeal this decision, please fill out the required information below and mail this form to the address shown below. A redetermination is the first level of the medicare appeals process. You need to provide your name, medicare number, date of service, date of notice, and reason. Download and complete this form to request a redetermination or clerical error reopening for medicare part b claims. Medicare part b redetermination and clerical error reopening request form. The form requires patient and provider. The form includes provider and beneficiary information, overpayment appeal, and. You need to provide your name, medicare number, date of service, date of notice, and reason for. This form may be used to request a redetermination for medicare part b services. Download and complete this form to appeal a medicare part b claim denial. The penalty is 10% of $185, which is $18.50. Find out the timeliness, filing options, form. You must add $18.50 for each year that you don’t. Original medicare (part a and b) eligibility and enrollment; Please complete each field on the form to ensure. You need to provide your name, medicare number, date of service, date of notice, and reason for appeal, and. Follow the instructions and select the appropriate options for your. Personalized choicesexpert guidancecompare medicare optionsshop plans online Use this form to appeal a medicare claim decision at the first level of appeal.
Fillable Part B Redetermination Request Form Level 1 printable pdf

Fillable Online Medicare Part B Redetermination and Clerical Error

What Is Medicare Redetermination

Form Cms20027 Medicare Redetermination Request Form, Form Cms20034

Form Cms20027 Medicare Redetermination Request Form, Form Cms20034
Redetermination/Reopening Form Tutorial JF Part B Noridian

Fillable Online Medicare Part B Jurisdiction 15 Redetermination Request

MediCal Redetermination for Medicare Beneficiaries

Medicare Savings Programs Application/redetermination (Qmb, Slmb, Almb

Redetermination Cook County Health
Trusted Companiesenrollment Optionsget Personalized Quotesfind Medicare Plans
Download And Print This Form To Appeal A Medicare Determination Decision On Your Claim.
Find The Form Name, Purpose And Link To Download The Redetermination.
Download And Submit This Form To Request A Redetermination Of A Medicare Claim Within 120 Days From The Date Of Receipt Of The Initial Determination.
Related Post: